
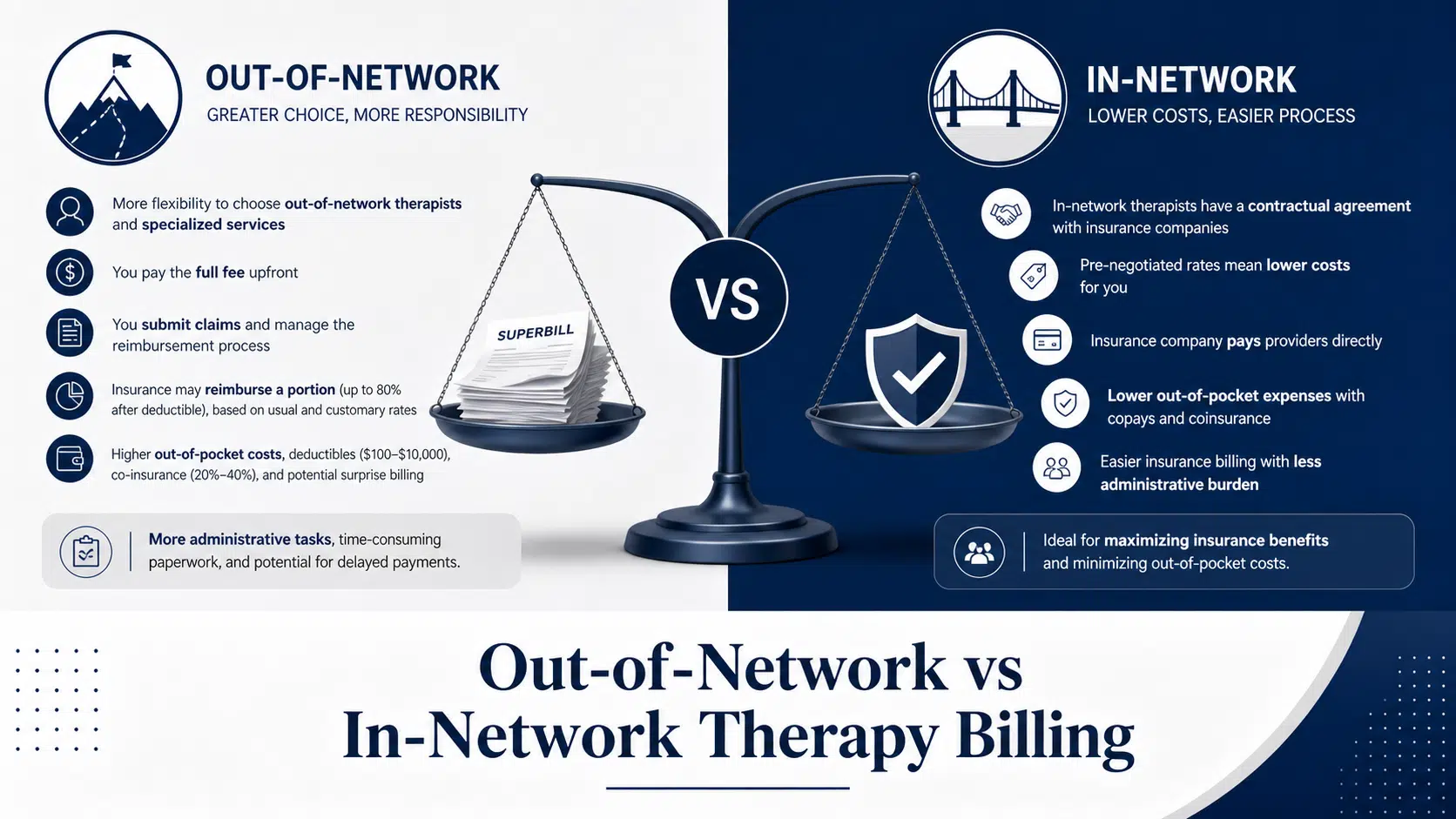
Out-of-Network vs In-Network Therapy Billing
10 min read
Behavioral Health Billing Errors: Avoidable Pitfalls Costing Your Practice Revenue Behavioral health and addiction treatment billing carries a higher error and denial rate than most medical specialties. At Cipher Billing, we see facilities losing 10–20% of collectible revenue to preventable billing
Cipher Admin
Cipher Billing Team

Behavioral Health Billing Errors: Avoidable Pitfalls Costing Your Practice Revenue Behavioral health and addiction treatment billing carries a higher error and denial rate than most medical specialties. At Cipher Billing, we see facilities losing 10–20% of collectible revenue to preventable billing
Behavioral health and addiction treatment billing carries a higher error and denial rate than most medical specialties. At Cipher Billing, we see facilities losing 10–20% of collectible revenue to preventable billing errors—money that should fund programs, staff, and patient services. Behavioral health providers face unique challenges in billing, coding, and reimbursement processes that set them apart from other healthcare sectors.
The landscape has shifted dramatically since 2020. Post-COVID telehealth policy changes in 2023–2025 created coding confusion. Medicaid redeterminations in 2024 caused coverage gaps for vulnerable populations. Meanwhile, parity enforcement has increased audit risk for mental health and SUD providers. These regulatory changes compound the already-complex billing requirements facing outpatient therapy, intensive outpatient (IOP), partial hospitalization (PHP), residential, and detox programs. Billing for behavioral health services is uniquely complex, often resulting in denial rates 85% higher than other medical specialties.
This article focuses on the concrete, recurring behavioral health billing errors we see across our clients’ claims data. We’ll cover the five most expensive mistake categories and show you how to fix them before they drain your cash flow.
Behavioral health and addiction treatment centers often face significant revenue losses due to five critical billing mistakes that drain financial resources. These errors include inadequate insurance verification leading to denied claims, incomplete or vague clinical documentation that fails to establish medical necessity, incorrect or outdated coding practices, late claim submissions missing strict filing deadlines, and ineffective denial management that allows recoverable payments to slip away. Each mistake not only reduces immediate reimbursements but also creates cascading administrative burdens, increasing days in accounts receivable and staff burnout. Identifying and correcting these common pitfalls is essential for behavioral health facilities to secure their revenue streams, improve cash flow, and reinvest in quality patient care and program development.
Mistake Category
Description
Impact on Revenue and Operations
How to Fix
Inadequate Insurance Verification
Failing to verify exact coverage, payer order, and carve-outs for behavioral health services
Denied claims mid-treatment, lost revenue, increased days in AR
Verify benefits at intake and regularly during treatment; document calls and use real-time eligibility tools
Incomplete or Vague Clinical Documentation
Notes failing to establish medical necessity or link symptoms to treatment interventions
High denial rates, downcoding, missed billing opportunities
Use standardized templates, document measurable goals and interventions, audit charts before claim submission
Incorrect or Outdated Coding Practices
Using wrong CPT/ICD-10 codes, missing modifiers, or outdated diagnostic codes
Claim denials, underpayments, compliance risks
Stay updated on coding changes, conduct coding audits, train staff on proper code use
Late Claim Submissions
Missing strict filing deadlines set by payers
Automatic denials, loss of reimbursement
Submit claims promptly, track deadlines with billing software, set internal SLAs
Ineffective Denial Management
Failing to analyze, appeal, and correct denials systematically
Write-offs of recoverable payments, cash flow disruption
Track denials by code and payer, use appeal templates, feed denial insights back into front-end processes
Before addressing specific errors, you need to recognize systemic warning signs in your revenue cycle.
Watch for these red flags:
A 32-bed residential SUD facility in Ohio discovered that 18% of charges were never collected due to preventable billing errors after we audited six months of claims. That’s six figures in annual revenue lost to fixable process failures.
These red flags point to repeatable breakdowns in eligibility, documentation, coding, submission, or follow-up—not random payer issues.
Faulty eligibility checks rank among the most expensive behavioral health billing challenges, especially for long episodes of care like 30–90 day residential or step-down programs. A single verification error at intake can result in an entire block of claims denied mid-treatment.
Common mistakes we see:
Billing the wrong payer due to incorrect payer hierarchy or failure to update primary and secondary payers is a frequent source of claim denials, often resulting in adjustments like PR 275.
Medicaid redetermination gaps in 2024 caused widespread CO 27 (expired coverage) and CO 31 (coverage gap) denials for patients whose eligibility lapsed during treatment. EAP visits incorrectly billed as primary insurance represent another frequent error—EAP is typically limited to brief interventions and should not be billed for residential stays.
Insurance verification and eligibility challenges are particularly pronounced in behavioral health, as patients often experience frequent changes in coverage that may go unreported, impacting billing and reimbursement.
You must verify benefits at intake and re-verify at fixed intervals (every 14 or 30 days) for residential, PHP, and IOP patients. Document call reference numbers and verified services. At Cipher Billing, we use real-time 270/271 eligibility tools plus manual payer calls for high-risk cases.
Behavioral health and addiction patients disproportionately experience job changes, Medicaid churn, and mid-year marketplace plan switches. This population has higher rates of employment instability and income volatility than general medical populations.
Typical coverage-change errors:
These mistakes trigger specific denial codes: CO 27 for expired coverage, B13 for coverage gaps, and PR 204 when benefit changes exclude covered services.
Operational fixes:
We routinely recover significant sums by correcting payer order and identifying retroactive Medicaid eligibility on older claims.
Missing, expired, or wrong-level authorizations represent one of the most preventable causes of behavioral health claim denials. Many payers require prior authorization for services such as residential treatment or partial hospitalization programs, and missing or delayed prior authorization can lead to claim denials.
Common authorization mistakes:
Many payers also require prior authorization for extended sessions or specialized care in behavioral health.
Payer requirements vary significantly. Aetna and Cigna required weekly reauthorization for residential in 2024–2025. Some plans limit IOP sessions to a fixed weekly count.
These errors generate CO 151 (authorization expired), CO 50 (not medically necessary at this frequency), and CO 109 (service not covered at this level) denials.
We recommend an authorization calendar with alerts 5–7 days before expiration and clear workflow assigning responsibility between utilization review and your billing team.
Behavioral health documentation faces scrutiny for medical necessity, functional impairment, and DSM-5/DSM-5-TR alignment. Vague progress notes are a major source of denied claims and downcoding. In mental health billing, using the correct CPT code for each behavioral health service is crucial, as accurate coding directly impacts claim approvals and reimbursement rates. Behavioral health billing is particularly complex due to the need for precise documentation that connects symptoms, diagnoses, and treatment approaches, with generic documentation often failing to meet medical necessity standards.
Documentation errors (what’s in the chart) and coding errors (what’s on the claim) feed into each other. Generic statements like “supportive therapy provided” do not establish medical necessity. At Cipher Billing, we audit charts for therapy, psychiatry, and MAT services before claims go out.
Services commonly denied for insufficient documentation:
Documentation gaps can lead to missed billing opportunities, especially for services such as assessment administration, treatment planning, and crisis services.
Phrases like “supportive therapy” or “client doing better” do not meet payers’ medical necessity standards for ongoing care.
Documentation patterns triggering CO 50 (medical necessity) and PR 32 denials:
A PHP program in 2025 improved approval rates by adding ASAM dimension checklists and LOCUS/CALOCUS scores to progress notes.
Structure for better notes:
We encourage standardized templates across clinicians to reduce variability and improve behavioral health coding accuracy.
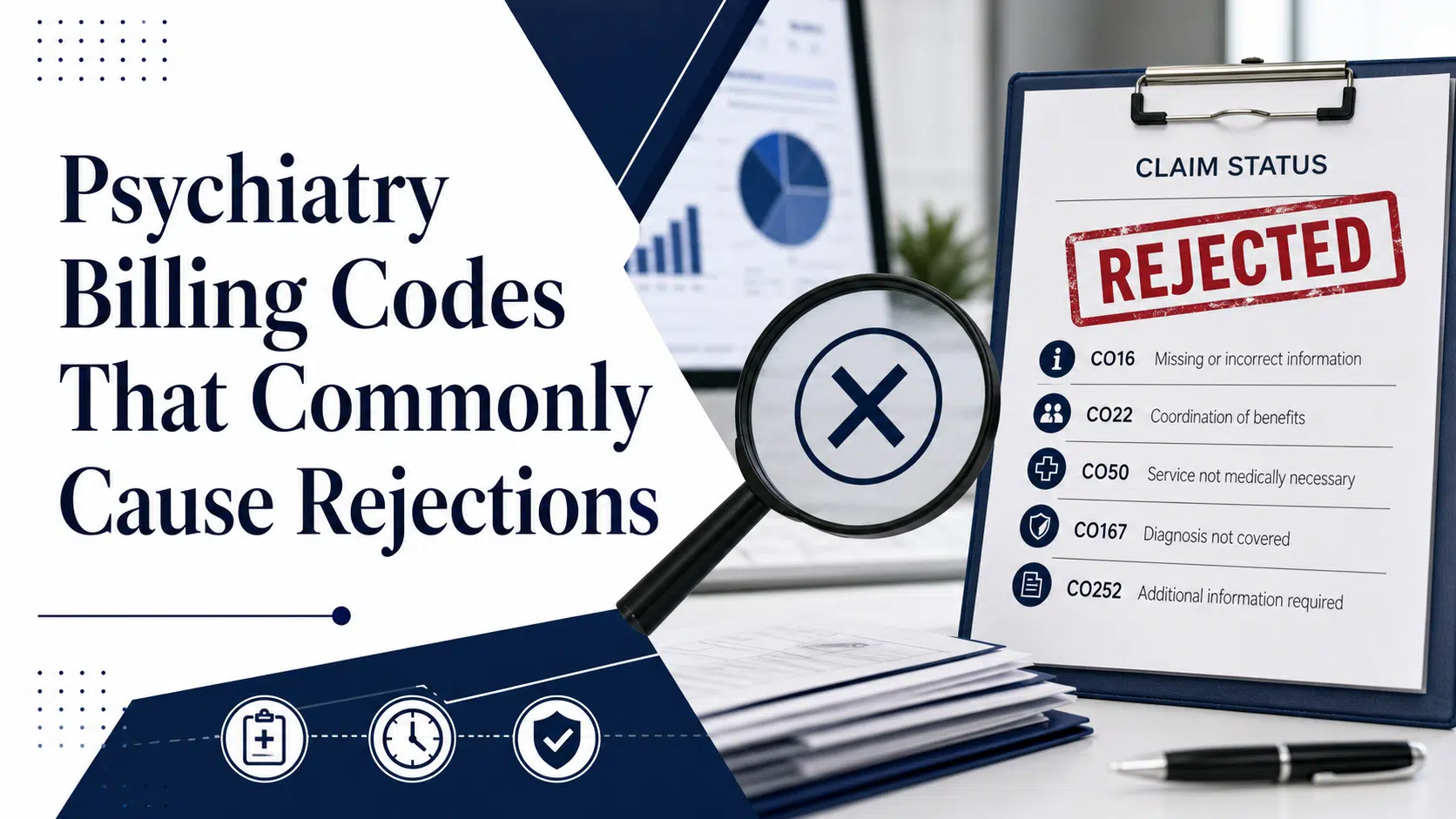
Behavioral health coding must reconcile CPT, ICD-10-CM, DSM-5-TR, and payer-specific restrictions—creating many opportunities for coding errors.
Recurring mistakes:
Uncovered diagnoses cause CO 167 (diagnosis uncovered) or CO 11 denials. The correct code matters.
Procedure-level errors:
Accurate use of service codes, especially for telehealth billing, is essential to ensure correct documentation and reimbursement. Using the right service codes, such as place of service codes, helps avoid claim denials and keeps your billing compliant with evolving regulations.
We use behavioral-health-specific coding audits and payer crosswalks to catch undercoding and mismatched code pairs before claims submission.
Telehealth expansion since 2020 led to payer-specific rules for POS codes and modifiers (02/10 plus 95 or GT). These billing mistakes remain common in 2025.
Common errors:
When billing for multiple services, such as individual and group therapy, on the same day within the same facility, it is essential to use the correct modifiers to avoid claim denials.
Florida Medicaid requires HE on certain behavioral services. California Medi-Cal uses U1 for peer support. Misuse causes CO 4 modifier denials.
Telehealth coverage tightened after the COVID-19 public health emergency ended in 2023. We maintain payer-specific modifier matrices updated quarterly to catch incorrect CPT codes.
Technically incorrect claims—wrong frequency codes, late filing, missing documentation, or duplicate submissions—drain revenue even when documentation and accurate coding are correct. Streamlining billing processes and adopting technology is essential to maintain steady cash flow for behavioral health providers.
Filing deadlines for most insurers are strict, often ranging from 30 to 180 days, and missing even one can lead to total loss of reimbursement.
Behavioral health practices with multiple levels of care (detox, residential, PHP, IOP, outpatient) are especially vulnerable due to complex billing rules and different billing entities (facility vs. professional claims). Many behavioral health practices struggle with this complexity.
We focus on front-end claim scrubbing and back-end payment reconciliation to prevent these errors from compounding month after month.
Behavioral health documentation delays, retroactive Medicaid approvals, and complex admissions often push claims against filing deadlines.
Common errors:
Industry estimates suggest up to 70% of CO 29 late filing denials are recoverable if appealed quickly with proper proof of timely submission.
Practical controls:
We routinely renegotiate timely filing language in payer contracts for new clients.
Improper rebilling is a frequent error when in-house teams try to “fix” problems by resubmitting claims without correct claim frequency codes.
Specific causes:
This triggers CO 18 (exact duplicate), CO 58 and CO 97 (already adjudicated), and B7 (prior payment issued) denials.
Coordination-of-benefits errors:
We use payer-specific COB rules and electronic EDI status checks to avoid duplicate submissions that trigger audits.
Inaccurate payment posting hides revenue leakage, underpayments, and missing secondary claims—especially damaging for thin-margin mental health providers.
Posting errors:
Residential programs missed out-of-network reimbursement increases after 2024 parity enforcement because underpayments were never identified in their billing system.
Best practices:
We provide monthly variance reports highlighting underpayments and trends in denial codes.
Denials are inevitable in behavioral health billing, but the real revenue loss occurs when organizations fail to analyze, appeal, and fix root causes through systematic denial management.
Many treatment centers treat denials as isolated “one-offs” instead of patterns, leading to avoidable write-offs and cash flow challenges.
We manage denials by grouping them by code, payer, and program type (e.g., MAT vs. residential) and building standard appeal templates for common behavioral health issues.
Many facilities simply post denials as adjustments without categorizing them by CO/PR codes, losing insight into systemic issues.
Denial codes behavioral health providers must monitor:
Simple tracking approach:
We recommend monthly denial review meetings focused on top 5 recurring codes rather than reviewing individual claims in isolation.
Many behavioral health claim denials are overturnable if appealed with strong clinical documentation and knowledge of parity rules.
Common appeal errors:
A Texas SUD clinic reversed a large share of CO 50 MAT denials by adding compliance data (UDS results, attendance logs) and citing SAMHSA TIP 63 and state parity requirements.
Structured appeal toolkit:
We track overturn rates so facilities can see ROI on appeal efforts.
Denial prevention requires intake, clinical, and billing teams to see the same patterns.
Examples of missed feedback loops:
Monthly feedback loop:
We often lead these review sessions, translating denial data into operational changes.
Beyond revenue loss, billing mistakes can trigger payer audits, recoupments, and regulatory scrutiny—especially around medical necessity, parity, and SUD confidentiality.
Addiction treatment centers face particular scrutiny from commercial insurance providers, state Medicaid programs, and occasionally the OIG due to historical fraud cases.
Payers and auditors use analytics to spot cloned notes and patterns of maximum-time codes without variation.
Repeated identical notes or unchanged treatment plans can appear as fraud, even if unintentional.
Controls:
We flag unusual patterns (e.g., 100% of therapy sessions billed at longest duration) and work with clinical leadership to correct documentation requirements before payers react.
MHPAEA requires mental health and SUD benefits be comparable to medical/surgical, but plans still legitimately exclude some services.
Non-covered services in behavioral health settings:
Errors arise from billing excluded services without financial agreements or mislabeling experimental services as standard psychotherapy.
When exclusions seem inconsistent with covered medical benefits, appeals can reference MHPAEA, state parity laws, and plan documents.
SUD programs are governed by 42 CFR Part 2, imposing stricter confidentiality rules than HIPAA—including for billing and sharing information with insurance companies.
Common errors:
Incomplete consent can trigger CO 16 denials or payer record requests that cannot be fulfilled without proper authorization.
We work with clients’ compliance officers to ensure billing documentation respects both revenue needs and Part 2 protections.
Maintaining steady cash flow is the backbone of financial stability for behavioral health practices. Cash flow challenges—such as delayed payments, denied claims, and inefficient billing processes—can quickly disrupt operations and threaten the quality of patient care. To overcome these obstacles, behavioral health providers must adopt a proactive, structured system for managing cash flow.
Start by regularly reviewing accounts receivable to identify outstanding balances and track claims status. Prompt follow-up on pending payments and denied claims is essential to prevent revenue from slipping through the cracks. Leveraging billing software that offers real-time updates on claim status and payment processing can significantly reduce cash flow issues and administrative burden.
A systematic approach to submitting claims, verifying benefits, and managing denials is crucial. By ensuring that claims are submitted accurately and on time, and by promptly addressing any denials, behavioral health practices can maintain a predictable revenue cycle. This allows providers to allocate resources efficiently, invest in staff and programs, and ultimately deliver better patient care.
In today’s complex behavioral health billing environment, prioritizing cash flow management is not optional—it’s essential for the long-term financial stability and success of your practice.
For behavioral health facilities aiming to achieve sustainable revenue growth, optimizing billing processes is a strategic imperative. The path to increased revenue begins with reducing preventable billing errors, strengthening coding practices, and ensuring thorough documentation for every service provided.
Implementing a robust billing platform can automate claims submission, verify insurance eligibility, and provide real-time claim status updates, all of which help reduce administrative burden and minimize common errors. Regular internal audits are invaluable for identifying issues such as incorrect CPT codes, missing documentation, and outdated codes—allowing for timely corrections and resubmission of clean claims.
Staying current with payer rules, diagnostic criteria, and coding guidelines is equally important. As insurance companies frequently update their requirements, behavioral health practices must adapt quickly to avoid denied claims and maximize reimbursement. Systematic denial management, supported by practice management systems, ensures that denied claims are addressed efficiently and that lessons learned are fed back into front-end processes.
By streamlining billing processes, behavioral health facilities can improve cash flow, reduce cash flow challenges, and dedicate more resources to patient care. Optimized billing not only supports compliance and financial health but also empowers mental health providers to focus on delivering high-quality behavioral health services without the distraction of ongoing revenue cycle headaches.
Cipher Billing exists specifically to solve the behavioral health billing errors described in this article. We combine specialized expertise, billing platform technology, and process design to reduce administrative burden.
Our core billing service offerings:
One client reduced days in AR from 70 to under 40 and cut denial rates by half within six months using our practice management systems integration.
Our team comes from behavioral health and addiction treatment backgrounds. We understand levels of care, ASAM diagnostic criteria, and payer rules specific to mental health practices and SUD behavioral health providers.
Ready to identify your revenue opportunities? Owners, CEOs, CFOs, and clinical directors of behavioral health and addiction treatment centers can schedule a consultation or billing audit to uncover your specific error patterns.
Behavioral health billing errors follow predictable patterns across eligibility, documentation, coding, claim submission, payment posting, and denial follow-up. Because they’re predictable, they’re fixable with the right structured system.
Reducing common errors doesn’t just improve revenue—it creates financial stability and steady cash flow so mental health providers can focus on patient care rather than constant cash flow issues.
Strong billing foundations now prepare you for changes ahead in 2026 and beyond, including evolving value-based models and shifting telehealth payer rules. Whether you conduct an internal audit or partner with a specialized billing service like Cipher Billing, the goal is the same: transform chaotic billing processes into a consistent, compliant revenue engine that supports your mission to deliver quality behavioral health services.
About the Author
Cipher Billing Team
In This Article
Cipher Billing specializes in behavioral health revenue cycle management. Reach out for a free consultation and see how we can maximize your reimbursements.
