
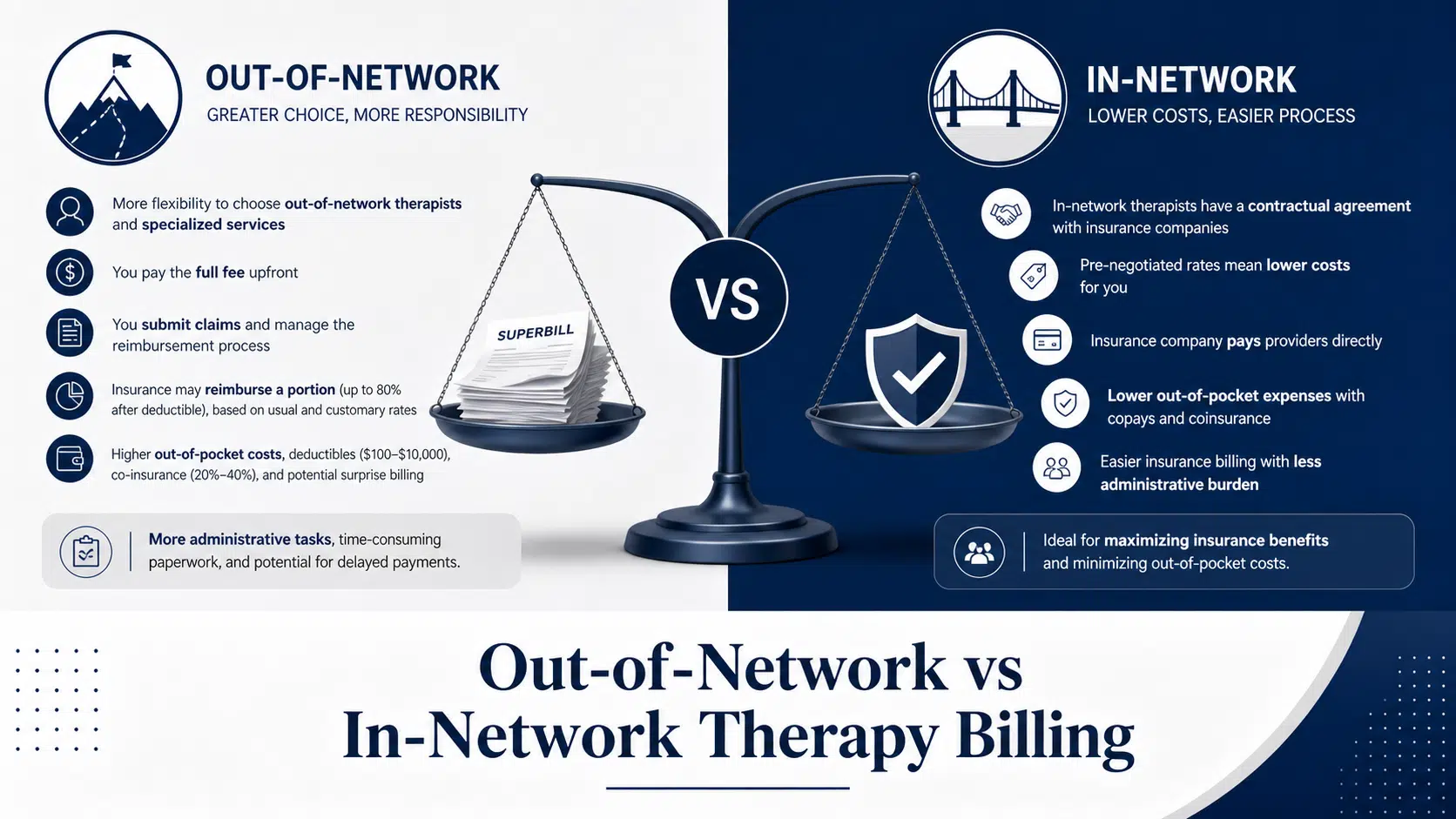
Out-of-Network vs In-Network Therapy Billing
10 min read
The behavioral health claims landscape in 2025 is fundamentally different from even two years ago. Pandemic-era flexibility has given way to permanent but stricter rules, and payers are scrutinizing documentation like never before. At Cipher Billing, we’re helping addiction and mental health facilit
Cipher Admin
Cipher Billing Team

The behavioral health claims landscape in 2025 is fundamentally different from even two years ago. Pandemic-era flexibility has given way to permanent but stricter rules, and payers are scrutinizing documentation like never before. At Cipher Billing, we’re helping addiction and mental health facilit
The behavioral health claims landscape in 2025 is fundamentally different from even two years ago. Pandemic-era flexibility has given way to permanent but stricter rules, and payers are scrutinizing documentation like never before. At Cipher Billing, we’re helping addiction and mental health facilities navigate these shifts daily—and the patterns are clear.
Demand for mental health services and addiction treatment remains elevated post-pandemic, with behavioral telehealth still representing roughly 30% of visits in many markets. The behavioral health market has expanded significantly, with outpatient visits reaching 40% of all visits in some measurement periods. This structural growth reflects genuine need—the United States continues experiencing a mental health crisis affecting people of all ages.
As the demand grows, the complexity of medical billing for behavioral health has also increased, especially due to the sensitivity and regulatory challenges associated with mental health conditions. Accurate billing practices are essential to ensure compliance and optimize revenue cycles in this evolving landscape.
Payers are also increasingly encouraging the integration of mental health with primary care, creating new billing opportunities for providers as collaborative care models become more common.
However, the claims environment has become considerably more complex. Medicare has moved from temporary waivers to permanent coverage with narrower technical requirements. Commercial plans are updating clinical policy bulletins with emphasis on evidence-based modalities, structured outcome tools, and stepped levels of care.
From Cipher Billing’s perspective, we see this show up at the claim level in specific ways: more chart requests, increased use of audits, and denial reasons shifting from “service not covered” to “documentation insufficient” or “medical necessity not established.” The behavioral health industry is experiencing a fundamental shift in how payors evaluate claims. There is also a shift toward value-based billing in mental health, prioritizing patient outcomes over service volume and aligning with the Medicare Access and CHIP Reauthorization Act (MACRA) and the Merit-Based Incentive Payment System (MIPS).
This article covers the main themes behavioral health providers must understand: telehealth policy shifts, new Medicare and commercial coding rules, parity enforcement, technology in billing, and denial prevention strategies tailored to mental health and addiction programs.
Telehealth remains central to behavioral health care and SUD treatment in 2025, but payors are moving from pandemic flexibility to permanent but narrower rules. Telehealth visits for behavioral health care grew from around 1% prior to 2020 to more than 32% in the first half of 2022, indicating a dramatic expansion in telehealth services. Medicare patients can permanently receive telehealth services for behavioral health in their home settings, but the technical requirements have tightened considerably.
Medicare’s 2025 stance includes:
Medicare now covers almost all behavioral health care through telehealth, allowing patients to access care from home and utilize audio-only visits, which has been a major shift in telehealth billing practices.
Practical claim details that cause problems:
Issue
Impact
Using POS 11 (office) instead of POS 02 (telehealth) or 55 (home)
Denial or underpayment
Missing modifier 95 or GT for synchronous video services
Downcoding or rejection
Audio-only services billed without checking payer coverage
Denial for non-covered modality
Missing telehealth consent documentation
Chart audit failure
The 2025 updates to CPT codes will require providers to document the technology platform used for telehealth services, including patient consent and any technical difficulties encountered during sessions.
Many commercial plans in 2025 have stricter rules on audio-only services for therapy-based CPT codes (90832-90838). What Medicare allows, a commercial plan may reject.
For hybrid models common in addiction treatment—in-person intake with telehealth follow-up groups—mixed-modality documentation must clearly distinguish between in-person and telehealth encounters. The 2025 CPT code revisions for psychotherapy codes (90832, 90834, 90837) will incorporate telehealth modifiers and refined documentation standards. Healthcare providers should maintain payer-specific telehealth matrices by CPT/HCPCS, modifier, and place-of-service, reviewing them quarterly as waivers phase out.
Medicare’s permanent extension of telehealth coverage for behavioral health has significantly increased access to mental health services.
The 2025 Medicare Physician Fee Schedule both expands behavioral health benefits and constrains reimbursement, forcing providers to be precise with accurate coding. There’s approximately 2-3% downward pressure on Medicare behavioral health reimbursement in 2025, with real margin impact for small mental health and addiction programs relying on Medicare and Medicare Advantage populations.
Key new or expanded HCPCS G-codes relevant to behavioral health:
OTP and MAT-specific changes include: flexibility for audio-only intake in some cases, remote counseling options, and increased emphasis on social determinants of health screening that can strengthen medical necessity arguments.
Mental health providers serving Medicare populations should conduct an early-2025 audit of superbills, EHR visit types, and charge masters to ensure compliance with all new behavioral health codes. Missing these billing processes updates leaves revenue on the table.
2025 solidifies digital tools as billable services when FDA-cleared and incorporated into treatment plans, but only with correct coding and documentation. Medicare now covers certain digital mental health devices and apps under new HCPCS codes like G0553 and G0554.
What payors want to see for digital therapeutics claims:
Remote therapeutic monitoring and remote patient monitoring codes apply to behavioral metrics like mood, adherence, cravings, and sleep. However, not all apps qualify—payors look for FDA clearance and clinician oversight. Consumer wellness apps (Calm, Headspace) cannot be billed using digital therapeutic codes.
From Cipher Billing’s perspective, behavioral health practices should create standardized EHR templates to capture PDT/RTM/RPM documentation, train clinicians on when to bill digital codes versus when they’re bundled into existing therapy visits, and monitor payer guidelines quarterly because commercial plans treat digital mental health differently than Medicare.
2025 sees intensified enforcement of the Mental Health Parity and Addiction Equity Act, with commercial health plans tightening utilization management while exposing themselves to parity audits. Federal regulations now require insurers to make prior authorizations, network availability, and care management services no more restrictive for behavioral health than for medical or surgical care.
How this plays out in claims and prior auth:
The 2024-2025 parity regulations require plans to demonstrate that non-quantitative treatment limits for behavioral health are comparable to those used for physical health services. This creates leverage for appeals when behavioral health claims are treated more harshly.
From Cipher Billing’s experience, we advise providers to:
As of early 2025, 29 states had enacted 75 bills addressing behavioral health coverage mandates, workforce issues, and crisis response—creating additional compliance requirements but also provider leverage.
The biggest claims risk in 2025 isn’t that services are “not covered”—it’s that they’re not documented and coded in the way payors now demand. Foundational CPT codes (90832-90838 psychotherapy; 90791/90792 psychiatric eval; 99202-99215 E/M) remain central but require precise pairing with correct time ranges, modifiers for telehealth or collaborative care, and accurate primary and secondary ICD-10-CM mental health diagnoses.
Common 2025 denial triggers Cipher Billing sees:
Denial Trigger
Root Cause
Telehealth claims rejected
Missing consent or modality documentation
Group/IOP sessions denied
Wrong place-of-service or unit errors
Medical necessity denials
Missing linkage between diagnosis and billed service
Authorization lapses
Expired or incomplete prior authorizations
Prior authorizations represent a growing pressure point. More services require auth (residential, intensive family therapy, psychological testing), with stricter proof-of-failed lower levels of care and shorter windows to submit clinical updates. Billing errors in this area lead directly to delayed payments or write-offs.
Recommended operational fixes:
Patient-centered care is at the forefront of the behavioral health industry, emphasizing the importance of tailored treatment plans and personalized support. In the context of behavioral health billing, patient-centered care translates to accurate and efficient claims processing, ensuring that patients receive the necessary mental health services without undue financial burden. Successful behavioral health billing relies on the alignment of claims with patient outcomes, necessitating a deep understanding of billing systems, regulatory changes, and the nuances of mental health support.
Behavioral health providers must navigate complex billing practices, balancing the need for comprehensive care management services with the requirements of insurance coverage and reimbursement processes. The Mental Health Parity and Addiction Equity Act has played a significant role in promoting equal coverage for mental health and physical health services, yet inconsistencies in payer policies and prior authorization requirements continue to pose challenges. Intensive outpatient programs, for instance, may be subject to varying levels of coverage, and billing professionals must be adept at confirming coverage details to minimize claim denials.
The integration of digital tools in behavioral health billing has been instrumental in streamlining processes, reducing billing errors, and enhancing patient engagement. Artificial intelligence, in particular, has shown promise in automating repetitive tasks and improving the accuracy of billing practices. However, human oversight remains essential to ensure compliance with regulatory changes and to address the complexities of mental health diagnoses and treatment plans.
As the behavioral health landscape continues to evolve, healthcare providers must stay abreast of developments in telehealth services, coding updates, and changes in insurance coverage. The expansion of telehealth access has been a significant trend, offering patients greater flexibility in accessing mental health care. Nonetheless, billing for telehealth services requires careful attention to payer guidelines, prior authorization requirements, and the nuances of Medicare patients’ coverage.
Inadequate documentation and coding errors remain common pitfalls in behavioral health billing, underscoring the need for certified coders and meticulous record-keeping. By prioritizing accurate billing practices and investing in staff training, behavioral health providers can reduce claim denials, expedite reimbursement, and focus on delivering high-quality patient care. Real-time eligibility verification and automated tracking of authorization statuses can also help mitigate payment delays and ensure seamless care transitions.
Ultimately, patient-centered care and billing in the behavioral health sector demand a holistic approach, one that balances the clinical and administrative aspects of care delivery. By embracing innovative billing solutions, fostering collaboration between healthcare providers and billing professionals, and advocating for patient-centric policies, the behavioral health industry can work towards a future where mental health services are accessible, affordable, and tailored to the unique needs of each individual. As the industry continues to navigate challenges and opportunities, the importance of patient consent, education, and engagement will only continue to grow, shaping the trajectory of behavioral health billing and care management services in the years to come.
Technology alone doesn’t fix claims problems—it must be combined with behavioral health billing expertise and refined billing operations. Successful behavioral health billing requires both automated tools and human oversight.
Key technology capabilities for 2025:
Regarding artificial intelligence and automation: use automated eligibility checks, prior auth status updates, and batch claim status queries. However, be cautious about auto-coding—behavioral health billing specialists with human review remain essential for complex SUD and dual-diagnosis cases to minimize claim denials and streamline processes.
From Cipher Billing’s viewpoint, a specialized billing partner helps by keeping pace with mid-year payer rule changes, providing ongoing training based on real denial data, and managing appeals aggressively with parity-focused arguments. Certified coders who understand behavioral health can identify coding errors that billing systems miss.
Here’s a step-by-step roadmap behavioral health practices can follow over the next 3-6 months:
Structured internal review:
Training priorities:
Policy and workflow updates:
Set measurable goals (reduce denial rate by X%, cut AR over 90 days by Y%) and consider engaging Cipher Billing to co-design and monitor metrics for your behavioral health and SUD programs. The challenges and opportunities in 2025 require both accurate billing practices and strategic partnership.
Providers should map which services currently depend on waivers, including home-based telehealth, audio-only options, and certain place-of-service codes. Contact each MAC and Medicare Advantage plan to confirm how they’ll handle telehealth starting Q4 2025 and into 2026. Build contingency plans now—shifting some patients back to in-person care, updating consent forms, and revising scheduling templates to avoid sudden coverage gaps. The telehealth expansion may narrow, so prepare your billing practices accordingly.
The most frequent denial reasons include missing or inconsistent time documentation for psychotherapy codes, telehealth claims lacking modality, platform, or consent notation, and medical necessity denials for higher levels of care where notes don’t clearly show failed lower levels or functional impairment. Lapsed or incomplete prior authorizations also drive significant claim denials, particularly for residential and PHP admissions. Inconsistent payer policies compound these issues across different insurance company products.
Small practices can manage if they designate a specific person to track payer bulletins and code updates monthly, use an EHR and billing systems configured for behavioral health, and limit panel diversity when possible to reduce complexity. However, many solo and small group mental health and SUD practices choose partners like Cipher Billing once time spent on appeals and tracking regulatory changes outweighs internal capacity. The administrative tasks burden often exceeds what small teams can handle while maintaining patient care quality and patient engagement.
Some payers in 2025 are adding bonuses and withholds tied to metrics like follow-up after hospitalization, reduced readmissions, and symptom score improvements. Claims still use CPT/HCPCS codes, but reporting requirements expand—capturing PHQ-9 scores, appointment adherence, and other health benefits measures. Providers should ensure their EHR can pull outcomes reports and that their billing partner understands how these metrics tie to reimbursement processes and insurance coverage incentives.
Gather 6-12 months of claims, payment, and denial reports by payer and level of care. Schedule a discovery call to review current workflows, payor mix, and top problem areas like residential, OTP, or IOP services. Allow Cipher Billing to perform a focused audit of sample denied claims and current documentation. Use those findings to decide between full outsourcing, hybrid support for denials and appeals only, or targeted training for in-house billing professionals. This approach helps establish the reimbursement processes that work best for your specific behavioral health landscape.
About the Author
Cipher Billing Team
In This Article
Cipher Billing specializes in behavioral health revenue cycle management. Reach out for a free consultation and see how we can maximize your reimbursements.
