
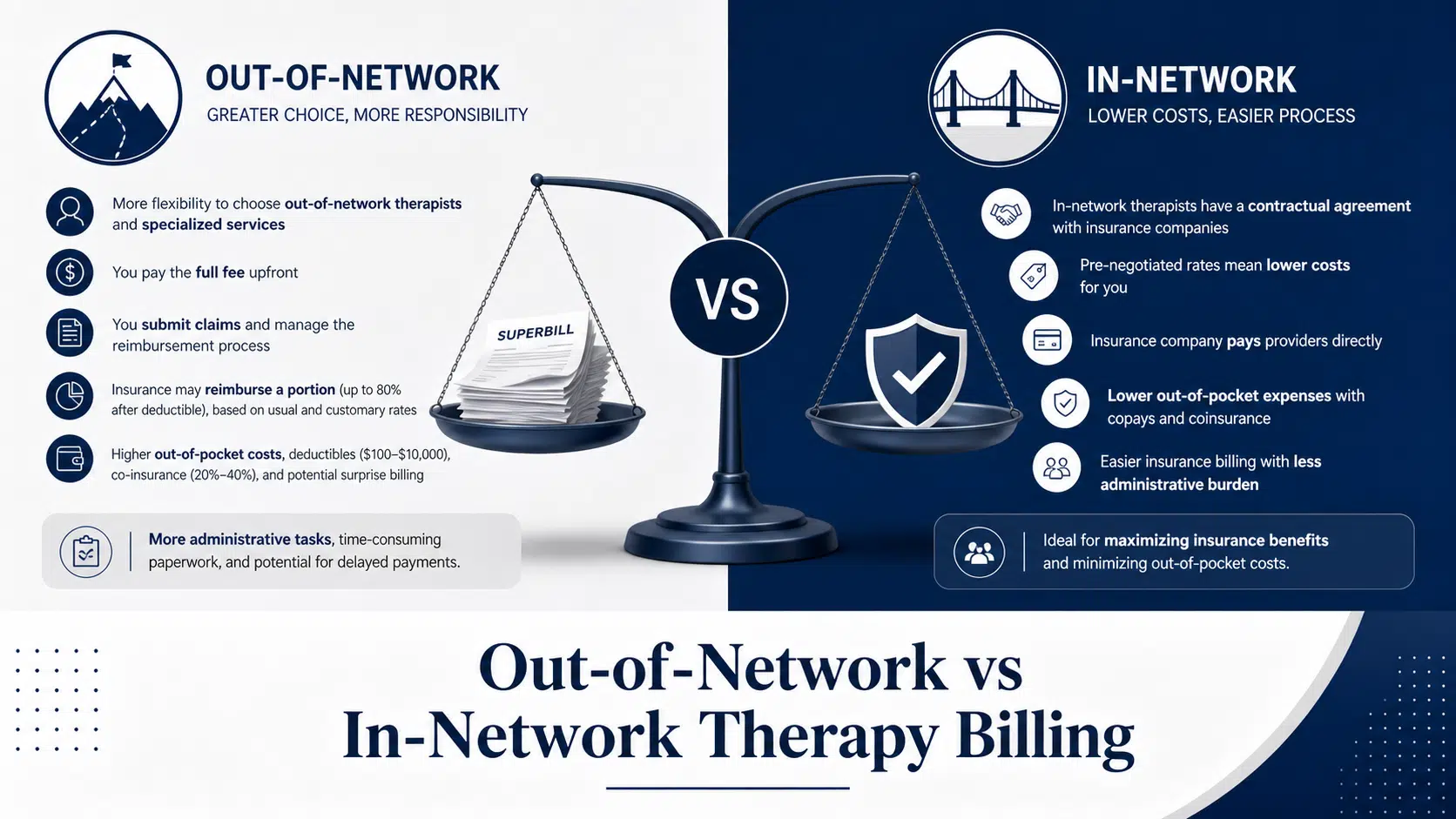
Out-of-Network vs In-Network Therapy Billing
10 min read
Key Takeaways The primary CPT codes for psychiatric diagnostic evaluation in 2026 are 90791 (without medical services) and 90792 (with medical services), while 96130–96133 support psychological testing evaluation services. CPT 90791 is used by non-prescribing clinicians such as clinical psychologist
Cipher Admin
Cipher Billing Team
Key Takeaways The primary CPT codes for psychiatric diagnostic evaluation in 2026 are 90791 (without medical services) and 90792 (with medical services), while 96130–96133 support psychological testing evaluation services. CPT 90791 is used by non-prescribing clinicians such as clinical psychologist
Understanding the correct cpt code for psych evaluation is foundational to behavioral health billing. In billing terms, a psychiatric evaluation refers to the comprehensive initial assessment that establishes diagnoses, informs treatment planning, and documents medical necessity for the entire episode of care. Get this wrong, and underpayment or denials can cascade through every subsequent claim.
As of 2026, the core intake and diagnostic codes remain 90791 for initial psychiatric diagnostic evaluation without medical services and 90792 for diagnostic evaluation with medical services. These codes are distinct from the 96130–96133 family, which covers psychological testing and neuropsychological testing evaluation—interpretive work following standardized test results rather than broad intake assessments. Confusing these code families is one of the fastest routes to claim denials.
Psychiatric evaluations anchor services rendered in substance use treatment, residential facilities, partial hospitalization programs (PHP), intensive outpatient programs (IOP), and outpatient mental health settings. Coding these evaluations correctly from admission sets the compliance tone for the entire patient stay. At Cipher Billing, we’ve focused exclusively on behavioral health billing since 2017, which means we track the frequent payer policy changes around these codes so facilities can focus on patient care instead of coding updates.
This section focuses specifically on the intake and diagnostic CPT codes used for psychiatric evaluations—not psychotherapy codes or psychological assessments administered via testing protocols.
CPT 90791 covers a comprehensive psychiatric diagnostic evaluation performed by non-prescribing clinicians. This includes:
The evaluation encompasses biopsychosocial history gathering, mental status examination (MSE), risk assessment for suicidality or violence, DSM-5-TR diagnostic formulation, and treatment planning. It explicitly excludes prescription writing, medication management, or independent medical assessment like lab orders or physical exams.
CPT 90792 applies to prescribers—psychiatrists, psychiatric nurse practitioners, and physician assistants—who incorporate medical decision making into the evaluation. Beyond the psychiatric assessment, 90792 documentation includes:
This code is appropriate for admission evaluations in detox, medication-assisted treatment (MAT), or substance use disorder programs where medical integration is central to clinical care.
Code
Medicare National Average
Commercial Payer Rates
90791
$150–$170
20–50% higher
90792
$160–$190
20–50% higher
Rates vary by state, payer mix, and geographic wage indices. Urban areas typically see uplifts while rural settings face downward adjustments.
Important: 90791 and 90792 are generally not reported together on the same date for the same patient by the same provider. Pairing with evaluation and management e/m codes requires distinct service separation to avoid bundling denials.
Accurate code selection between 90791 and 90792 is one of the most frequent audit targets in behavioral health billing. Payers recover significant revenue when facilities bill 90792 without documented medical services, downcoding to 90791 and recouping the difference—sometimes 10–30% per claim in audited practices.
Use 90791 when:
Use 90792 when:
Example 1: IOP Therapist Intake A licensed clinical social worker conducts a 60-minute intake on a new patient with anxiety and trauma history. The evaluation includes comprehensive biopsychosocial history, MSE noting coherent thought process and low suicide risk, DSM-5-TR diagnosis of F41.1 (generalized anxiety disorder), and initial treatment planning. Bill 90791.
Example 2: Psychiatrist MAT Evaluation The same patient later sees a psychiatrist for benzodiazepine evaluation. The psychiatrist documents medical history, reviews ECG for cardiac risks, assesses medication interactions with the patient’s current prescriptions, and develops a medication plan. Bill 90792.
Example 3: Detox Admission A psychiatric NP performs an admission evaluation for a patient entering detox for opioid use disorder. Documentation includes physical exam findings, liver function test review for psychotropic clearance, polypharmacy risk assessment, and MAT initiation plan. Bill 90792.
If medical services are minimal or undocumented, payers will downcode 90792 to 90791, resulting in revenue loss and potential compliance risk.
Although 90791 and 90792 are not formally time based codes like psychotherapy, payers increasingly expect reasonable encounter lengths (typically 45–90 minutes) and robust documentation to justify reimbursement.
A compliant psychiatric evaluation note should include:
When billing 90792, documentation must also include:
CPT 90792 is intended for comprehensive initial evaluation—not routine medication checks. For follow-up medication management visits, use evaluation and management codes (99212–99215) based on time or medical decision making complexity.
If a provider bills both an e m service and a same-day psychotherapy add-on (90833/90836/90838), modifier 25 is required for significant, separately identifiable work. However, 90791/90792 typically stand alone for primary psych evaluations and should not be paired with E/M for the same problem without clear clinical separation.
Broad psychiatric diagnostic evaluations (90791/90792) differ fundamentally from testing-focused psychological testing evaluation services that rely on the 96130–96133 code family.
These codes capture integrating clinical data from psychological assessments: test selection, record review, scoring, interpretation, report writing, and interactive feedback to patients and family members.
Neuropsychological test administration and evaluation focus on cognitive domains—memory, executive function, attention—relevant to dementia, traumatic brain injury, or cognitive disorder assessments.
The 96130–96133 family covers non-face to face services professional effort:
These codes do not capture raw test administration time, which uses separate codes (96136–96139).
Caution: Facilities frequently misuse 96130–96133 as generic “psych eval codes.” This triggers denials when the work overlaps with intake/diagnostic services that should use 90791/90792. Differentiate clearly between initial evaluation and testing-related evaluations for compliance.
Many payers and healthcare providers confuse screening and test administration codes with full psychiatric evaluations, causing denials and recoupments.
Code
Description
Approximate Rate
96136
First 30 min, provider-administered
$43.94
+96137
Each additional 30 min, provider
Add-on
96138
First 30 min, technician-administered
$37.73
+96139
Each additional 30 min, technician
Add-on
Minimum threshold is 16 minutes for the first unit. These codes apply when two or more tests are administered.
Screening, test administration, and evaluation services represent distinct stages of the assessment workflow:
Key rules:
Since the expansion of telehealth policies through CMS updates in January 2026, most major payers allow psychiatric evaluations via telehealth with specific modifier and place-of-service requirements.
CPT 90791 and 90792 remain on the Medicare telehealth list in 2026, reimbursed at in-person parity when billed correctly. Related codes 96127, 96130, 96136, and 96138 are also approved for telehealth delivery.
Element
Requirement
Modifiers
95 or GT
Place of Service
02 (non-home) or 10 (home)
Documentation
Audio-visual consent, patient location, clinical rationale
For psychological testing delivered via telehealth, documentation must confirm standardized tools are tele-compatible and include written reports.
Cipher Billing’s rapid VOB (8–9 minutes) is especially valuable for telehealth intakes. Same-day eligibility verification prevents denied psych evaluation claims before they occur.
This section serves as a practical checklist for billing and coding teams to prevent denials on psych evaluation codes in 2026.
Modifier 25: Use when a distinct, separately identifiable psychiatric evaluation occurs on the same day as an office visits medical encounter. Documentation must clearly delineate the services rendered temporally and clinically.
Telehealth modifiers (95/GT): Required for telehealth delivery; policies differ between Medicare, Medicaid, and commercial payers.
Scenario: A psychiatrist performs an initial MAT evaluation but documents only medication selection without comprehensive psychiatric assessment, MSE, or risk assessment. Payer downcodes 90792 to 90791, recouping the difference.
Prevention: Document full psychiatric diagnostic evaluation elements plus medical services component—systems review, lab integration, and medication decision making.
Scenario: An IOP bills 90791 on the same date as 99213 for the same presenting problem without modifier 25 or distinct documentation. Claim denied for bundling.
Prevention: Ensure appropriate codes are selected, documentation clearly separates the distinct service, and modifier 25 is applied when justified.
Payers increasingly perform post-payment audits on psych evaluations, focusing on medical necessity and whether the medical record supports the billed CPT code and complexity level.
For 96130–96133 and related codes:
Adopt structured note templates aligned with payer requirements. Conduct periodic internal audits before claims submission. Cipher Billing uses prospective chart audits during onboarding to identify missing elements before claims go out—catching coding practices issues that would otherwise result in denials or prior authorization delays.
Cipher Billing is a behavioral health-only RCM partner serving addiction treatment centers, residential facilities, PHP, IOP, and outpatient practices nationwide since 2017. Our exclusive focus on behavioral health means we understand the nuances of psych evaluation billing that generalist billing companies miss.
During onboarding, we review existing psych evaluation notes to align 90791/90792 and testing code usage with current payer policies. This prospective audit approach catches documentation gaps before they become denials—reducing revenue loss from the first month.
Metric
Cipher Performance
First-pass medical record approval
96%
Medical necessity appeal success
97%
Write-off rate
1.88%
VOB turnaround
8–9 minutes
Payer policies around psych evaluation billing, telehealth requirements, and modifier use change constantly. Cipher tracks these updates daily so providers can focus on clinical care instead of accurate coding updates. Our dedicated Partner Experience Executives—U.S.-based, not outsourced call centers—ensure facilities receive personalized support.
Ready to improve your psych evaluation reimbursement? Contact Cipher Billing at (949) 368-0575, email info@cipherbilling.com, or visit CipherBilling.com for a review of your current denial rates and potential revenue recovery opportunities.
For a single provider and single encounter, 90791 and 90792 are not billed together. Payers expect one primary psychiatric diagnostic evaluation code per patient per date of service.
In rare team-based assessments—such as a separate non-prescriber (LCSW) and prescriber (psychiatrist) conducting distinct evaluations on the same date—some payers may allow both codes with clear documentation and separate notes. This is payer-specific and requires verification before billing. Use Cipher Billing or internal compliance teams to confirm any exceptions.
CPT 90791 and 90792 are intended for initial or re-admission evaluations, not routine follow-ups. Frequency limits vary by payer and program type—UnitedHealthcare, for example, often limits to one per episode without documented medical necessity.
Some payers permit a repeat psychiatric evaluation when there is a major change in clinical status (psychosis emergence, new diagnosis, level-of-care transition) that justifies further evaluation. Document clearly why the comprehensive assessment is medically necessary, referencing payer manuals for specific frequency guidelines.
Psychiatric evaluations require mental or behavioral health diagnosis codes (ICD-10-CM F-codes) or relevant substance use conditions. Common examples include:
The diagnosis must be supported by history, mental status exam, and clinical formulation in the note. Some payers restrict “rule-out” diagnoses—document provisional diagnoses appropriately and follow payer-specific rules.
Medicare and many commercial payer rates reimburse 90791 and 90792 at parity with in-person rates in 2026 when billed with correct telehealth modifiers (95 or GT) and place-of-service codes.
Medicaid parity varies by state—some still pay different rates or restrict telehealth settings. Always verify payer-specific telehealth policies before new patient visits. Documentation must include audio-visual connection confirmation, patient location, and informed consent.
CPT 90792 is reserved for comprehensive initial psychiatric diagnostic evaluation that includes medical services. Ongoing medication management visits—reviewing response to treatment, adjusting medications, monitoring side effects—typically use E/M codes (99211–99215) based on time or medical decision making.
If the encounter focuses primarily on follow-up med management rather than comprehensive diagnostic assessment, an E/M code is usually more appropriate than repeating 90792. Follow organizational policy and payer guidance. When uncertain about code selection, consult with billing partners like Cipher Billing to ensure accurate coding and avoid audits.
About the Author
Cipher Billing Team
In This Article
Cipher Billing specializes in behavioral health revenue cycle management. Reach out for a free consultation and see how we can maximize your reimbursements.
