

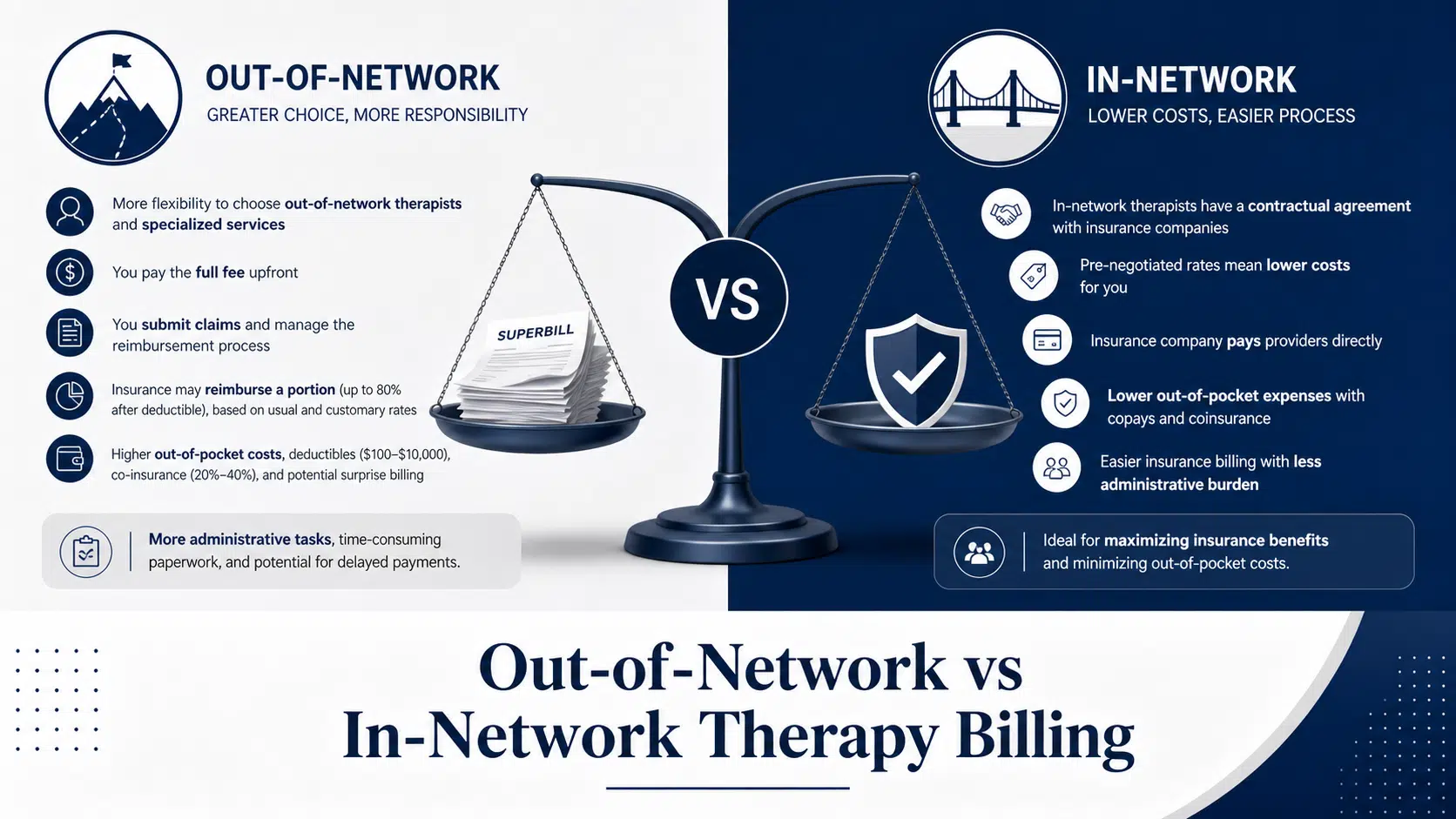
Out-of-Network vs In-Network Therapy Billing
10 min read
Behavioral health billing is a minefield. One missing modifier, one mistimed session note, one outdated diagnosis code — and your reimbursement vanishes into the abyss of insurance claim denials. For psychiatric and behavioral health providers, this isn’t just an annoyance; it’s a direct
Cipher Admin
Cipher Billing Team
Behavioral health billing is a minefield. One missing modifier, one mistimed session note, one outdated diagnosis code — and your reimbursement vanishes into the abyss of insurance claim denials. For psychiatric and behavioral health providers, this isn’t just an annoyance; it’s a direct
Behavioral health billing is a minefield. One missing modifier, one mistimed session note, one outdated diagnosis code — and your reimbursement vanishes into the abyss of insurance claim denials. For psychiatric and behavioral health providers, this isn’t just an annoyance; it’s a direct hit to your revenue cycle, your cash flow, and ultimately, your ability to deliver consistent patient care.
In this comprehensive guide, we’re breaking down the psychiatry billing codes that commonly cause rejections, the denial codes you’ll encounter most often, and the proven strategies to maintain compliance, reduce denied claims, and keep your practice financially healthy.
Mental health billing is uniquely complex. Unlike standard medical billing, behavioral health claims involve time based codes, strict documentation requirements, prior authorization hurdles, and payer specific policies that change constantly. According to the American Medical Association, CPT updates happen annually, and behavioral health is among the specialties most affected by yearly revisions.
Roughly 30% of behavioral health claims face delays or denials due to coding errors. That’s nearly one in three claims that never get paid on the first submission. For a busy outpatient mental health clinic or residential treatment facility, that statistic translates into hundreds of thousands of dollars in delayed or lost reimbursement annually.
Insurance claim denials in behavioral health have been rising due to stringent insurance policies and complex billing requirements. Even with the Mental Health Parity and Addiction Equity Act (MHPAEA) in place — which requires insurers to treat mental health services on equal footing with physical health services — providers still face disproportionate scrutiny on mental health claims.
Let’s get specific. These are the mental health cpt codes that consistently lead to claim denials when documentation, time tracking, or modifiers fall short.
This is arguably the most flagged code in all of behavioral health. Insurance payers scrutinize 90837 heavily because it pays more than its shorter counterpart, 90834. Without detailed documentation supporting an actual session length of 53+ minutes, expect claims denied or audited.
Used when session duration falls between 38 and 52 minutes. Using the wrong psychotherapy CPT code, even by a few minutes in session length, can trigger denials due to lack of supporting documentation.
The intake assessment code. It can only be billed once per patient per provider, per episode of care in most cases. Submitting claims for 90791 multiple times, or pairing it incorrectly with therapy codes on the same day, leads to instant rejection.
Reserved for prescribers. Frequently denied when billed by non-medical providers or without proper coding documentation showing the medical component.
These add on codes are billed alongside E/M codes (like 99213 or 99214) when a psychiatrist provides medication management plus psychotherapy in the same visit. Improper use of add on codes — including missing the primary E/M code — is a top denial driver.
This is one of the most asked questions in mental health billing. The short answer:
You cannot bill 90791 every visit. It’s an intake code. Confusing the two is one of the most common billing errors that lead to claim denials.
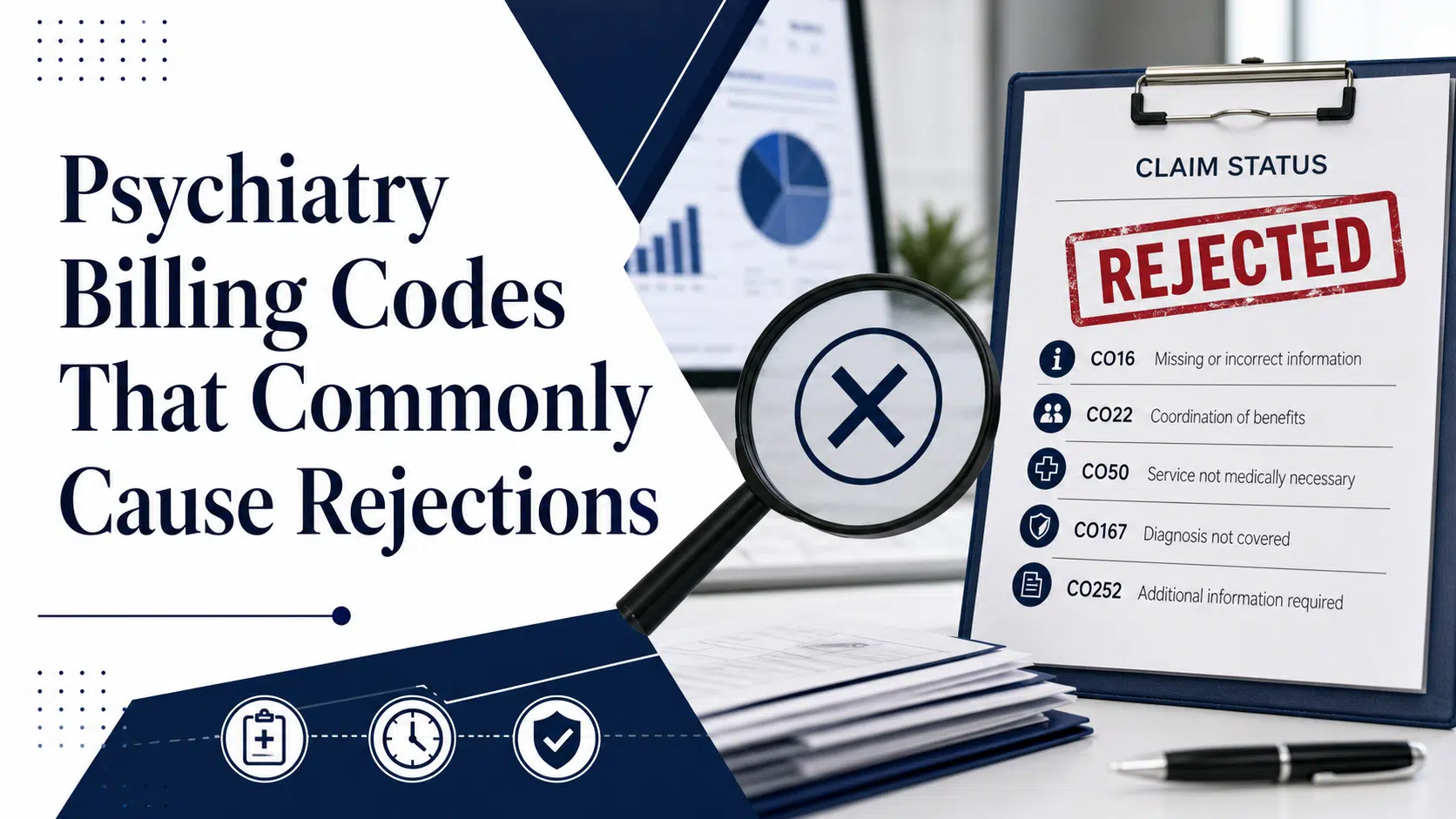
Understanding claim adjustment reason codes (CARCs) and remittance advice remark codes (RARCs) is essential to decoding why claims bounce back. Here are the top denial codes you’ll see on behavioral health remittances:
CO252 indicates the payer needs additional supporting documentation — usually clinical notes, treatment plans, or progress documentation — before they’ll process the claim. It’s not a final denial; it’s a request. Respond quickly with the requested clinical documentation to convert it into a paid claim.
So what are the most common coding errors resulting in denials? Based on industry data and our experience auditing thousands of behavioral health claims at Cipher Billing, here are the worst offenders:
A mismatch between diagnosis codes and procedure codes often leads to denials. For example, billing 90837 with an unspecified F code like F99 will rarely fly. Insurers want specificity. Using outdated, incorrect, or non-specific ICD-10 f codes is a denial magnet.
Failing to document exact start and end times for psychotherapy sessions is a major cause of denial in psychiatry billing. For all time based codes, the actual session length must be documented in the progress notes — not just “approximately 60 minutes.”
Missing modifiers for telehealth (95, GT) or for behavioral health service distinctions cause instant rejections. The CMS telehealth billing guidance outlines exactly which modifiers belong on virtual sessions.
Billing 90833 without a primary E/M code, or stacking add-ons incorrectly, will fail every time.
Vague or incomplete notes regarding progress, risk assessment, and treatment plans lead to denials because documentation must clearly support the billed code.
Accurate documentation is crucial in mental health billing as it directly impacts the approval of claims. Missing documentation is consistently cited as a leading cause of denials across behavioral health providers.
To document medical necessity properly, every chart should include:
Insurers require proof that services provided are necessary. Without it, expect a CO50. The American Psychological Association’s coding guidance emphasizes that documentation must clearly demonstrate medical necessity for every billed code.
Many commercial plans require prior authorization for intensive or longer-term therapy, residential treatment, PHP, and IOP services. Missing this step can lead to claim denials even if every other element is perfect.
Always verify eligibility AND verify coverage requirements before the first session. Confirm active coverage, copay, deductible status, and authorization requirements. At Cipher Billing, we deliver full VOB in 8–9 minutes — well below the industry standard of 30 — so admissions never stall.
Denial Code CO31 means the patient was not eligible on the date of service. This often happens with terminated coverage mid-treatment or Medicaid eligibility gaps. The fix:
Since 2020, telehealth volume in behavioral health has exploded — and so have telehealth-specific denial patterns. Common issues include:
Crisis services codes (90839, 90840) are some of the most under-utilized and most denied in psychiatry. They require detailed documentation of the crisis nature, urgency, and time spent. Use them only when truly indicated, and document accordingly.
When facing claim denials, don’t write off the revenue. Appeal aggressively. Here’s the playbook we use at Cipher to achieve a 97% medical necessity appeal success rate:
Smart practices track denial trends monthly. Identify your most frequent denial codes, categorize them by payer, and address the root cause. Are 30% of your denials CO50? You have a medical necessity documentation problem. Are 25% CO16? Your front-end data capture needs work.
Modern billing software can auto-generate denial pattern reports. According to CMS billing manuals, providers who actively monitor denial patterns recover 40% more revenue than those who don’t.
Beyond psychotherapy, providers frequently bill general mental health codes for testing, screening, and assessment (96130–96139). These require precise time documentation and proper coding sequencing. Improper unit billing here is a top audit trigger.
Denial Code CO22 hits when payers disagree on who’s primary. Common scenarios:
Always confirm COB status during VOB to avoid this.
Family therapy codes (90846 without patient present, 90847 with patient present) require documentation of who attended, the therapeutic focus, and how the session supports the identified patient’s treatment plan. Missing the participant identification triggers CO16 every time.
Errors in billing processes can be drastically reduced through:
At Cipher Billing, we’ve operated exclusively in denial prevention and behavioral health billing since 2017. Our approach to ensure proper billing combines:
We don’t just push claims. We fight denials, negotiate aggressively for out-of-network reimbursement (averaging 30.36%), and escalate to state insurance commissioners when necessary to protect your revenue.
Mental health providers shouldn’t lose sleep over coding minutiae. With proper documentation, proper billing workflows, and a partner who knows behavioral health inside and out, claim denials become the exception — not the rule.
Whether you’re running a high-volume outpatient practice, an IOP, PHP, or a residential treatment center, the principles are the same: detailed documentation, correct codes, accurate time tracking, and aggressive denial management. Get those right, and your behavioral health claims will be paid faster, more often, and at higher rates.
Ready to stop bleeding revenue to preventable rejections? Contact Cipher Billing at (949) 368-0575 or info@cipherbilling.com to schedule a free audit. A Higher Level Partnership starts here.
About the Author
Cipher Billing Team
In This Article
Cipher Billing specializes in behavioral health revenue cycle management. Reach out for a free consultation and see how we can maximize your reimbursements.
